A Meta-Analysis of Intraoperative Indocyanine Green vs Intraoperative Cholangiography for Bile Duct Stone Diagnosis in Laparoscopic Cholecystectomy Intraoperative Indocyanine Green vs Intraoperative Cholangiography

Article Sidebar
Abstract
Background: Laparoscopic cholecystectomy is one of the most common surgical procedures for the treatment of symptomatic gallstones. However, the presence of common bile duct stones (CBDS) increases the risk of complications and demands further diagnostic and therapeutic interventions. Currently, both intraoperative cholangiography (IOC) and intraoperative indocyanine green (ICG) fluorescence imaging are utilized for diagnosing CBDS during laparoscopic cholecystectomy. Yet, which of the two methods provides a higher diagnostic accuracy remains unclear.
Objective: This meta-analysis aims to compare the diagnostic accuracy of ICG fluorescence imaging and IOC for detecting CBDS during laparoscopic cholecystectomy.
Methods: The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were employed for the literature search, selection, and analysis of 12 studies involving 1973 patients. Summary estimates of the sensitivity, specificity, positive and negative likelihood ratios (LR+ and LR-), and diagnostic odds ratio (DOR) were calculated, as well as subgroup and sensitivity analyses. Egger's test and funnel plots were applied to assess publication bias and Cochrane's Q test and I^2 statistic to measure heterogeneity. Statistical analyses were performed using STATA software.
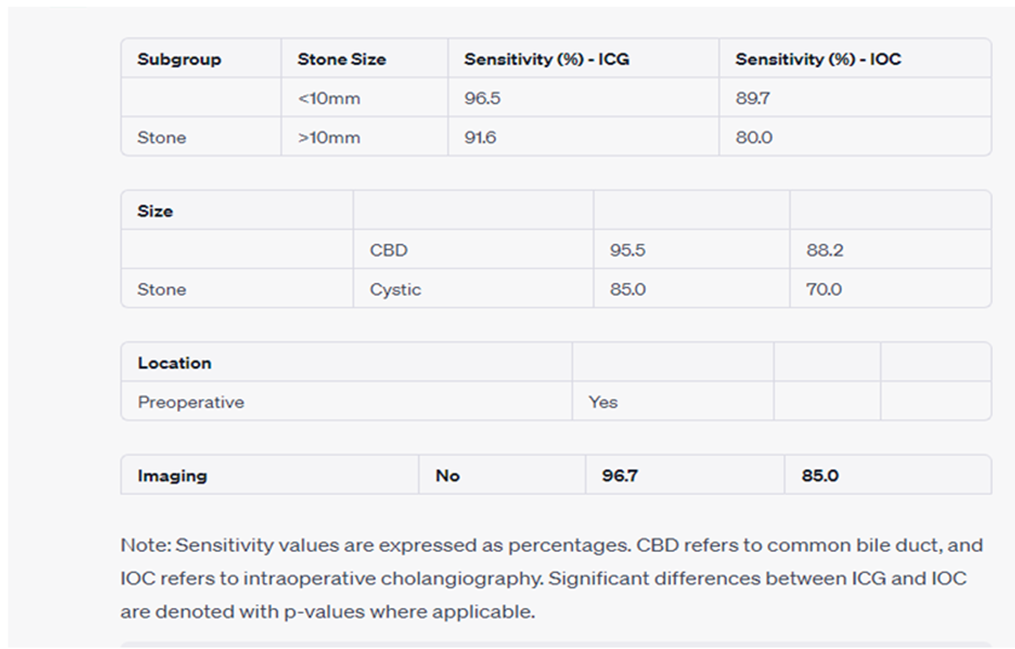
Results: The pooled results demonstrated a higher sensitivity and DOR of ICG fluorescence imaging (95% and 20.2, respectively) compared to IOC (87.5% and 9.2, respectively). The specificity was similar between the two methods (ICG: 96.1%; IOC: 97.5%). The LR+ was 35.3 for ICG and 35 for IOC, whereas the LR- was 0.06 for ICG and 0.13 for IOC. The subgroup analysis revealed no significant differences in sensitivity between the methods regarding stone size and location, while ICG was significantly superior to IOC in detecting CBDS in the absence of preoperative imaging. The sensitivity analysis showed the robustness of the results, and Egger's test and funnel plot suggested low risk of publication bias.
Conclusion: Intraoperative indocyanine green fluorescence imaging may possess a higher diagnostic accuracy than intraoperative cholangiography for identifying common bile duct stones during laparoscopic cholecystectomy. This finding should be considered in clinical decision-making and future research.